Treatment is based on any underlying causes (if known), any risk factors present, and the stage at the time of diagnosis. There isn't a one best treatment known for adhesive capsulitis. Studies done so far just haven't been able to come to a single evidence based set of treatment guidelines for this problem.
Nonsurgical Treatment
Treatment of adhesive capsulitis can be frustrating and slow. Most cases eventually improve, but the process may take many months. The goal of your initial treatment is to decrease inflammation and increase the range of motion of the shoulder. Your doctor will probably recommend anti-inflammatory medications, such as aspirin and ibuprofen.
During the early stage, your doctor may also recommend an injection of cortisone together with a long acting anesthetic, similar to lidocaine, to get the inflammation under control. Cortisone is a steroid that is very effective at reducing inflammation. Controlling the inflammation relieves some pain and allows the stretching programme to be more effective.
Nonsurgical Rehabilitation
Physiotherapy treatments at Physio Med are a critical part of recovery and rehab from this injury. The first goal is to reduce pain and interrupt the inflammatory cycle. Next our treatments are directed at getting the muscles to relax in order to help you regain the motion and function of your shoulder. The overall goal of Physiotherapy is to help you regain full range of motion in the shoulder.
If your pain is too strong at first to begin working on shoulder movement, your Physiotherapist may need to start with treatments that focus on pain control. The use of ice, heat, ultrasound, and other electrical modalities may be useful at this stage. Your therapist may also use massage and gentle mobilisations to ease muscle spasm and pain.
As soon as possible your therapist will begin to work on regaining your shoulder's movement, even if that range of movement is only small at first. Your sessions may begin with treatments such as moist hot packs, ultrasound or massage, which help to relax the muscles and get the shoulder tissues ready to be stretched. Your Physiotherapist will assist you in stretching your shoulder through the available ranges of motion, but they will also show you stretches that you can do on your own as part of a home programme. Using an overhead shoulder pulley in the clinic and as part of a home programme is extremely useful in gaining shoulder range of motion. Doing pendular exercises can also assist with pain at this stage, and help to maintain some shoulder range of motion. Pendular exercises are performed by leaning forward or to the side, letting the arm hang clear of the chest, and then initiating movement with your trunk so that the dangling limb passively and gently moves. This action provides some traction to the glenohumeral joint (shoulder joint), which aids in pain relief, and also assists the shoulder into a relative elevated motion (in relation to the trunk.) It is important that the pendular activity is done as passively as possible without initiating motion from the shoulder muscles. The exercise should look similar to a weighted pendulum that randomly swings on the end of a piece of string.
If your Doctor recommends an injection of a long acting anesthetic with cortisone for your shoulder, you should plan on seeing your Physiotherapist at Physio Med 4 days after the injection.
Maintaining your neck range of motion is also very important when your shoulder is not moving well, so your therapist will also prescribe exercises to ensure you can move your neck well for all your daily activities, and that you don't end up with a stiff neck along with your stiff shoulder.
The next part of your treatment at Physio Med will involve mobilising the joints of your shoulder, including your glenohumeral joint, the joint of the shoulder blade and the thorax (scapulothoracic joint), and even the joints where your collarbone joins the trunk and the shoulder (sternoclavicular and acromioclavicular joints.) Your Physiotherapist will passively move these joints into their available ranges of motion while you relax the muscles of your shoulder completely.
Interestingly, the strength of your shoulder is often maintained in primary adhesive capsulitis, especially once you pass the stage of having pain and are simply restricted because of the range of motion. As you gain more range of motion, however, you will notice weakness in the shoulder in these ranges of movement simply because you have not used the shoulder in these ranges for an extended period of time. For this reason, your therapist will focus more on strengthening exercises in the later stages of your rehabilitation, once your pain is under control and your shoulder range of movement is improving.
With secondary adhesive capsulitis there may be significant weakness in the shoulder due to the original injury that started the process in the first place (i.e. shoulder impingement or rotator cuff tear.) In these cases, your therapist will start by prescribing simple strengthening exercises. Initially this will only involve isometric strengthening. Isometric strengthening exercises are done by tightening your muscles without actually moving the associated joint. Isometric exercises work the muscles without straining the injured or painful tissues. Your Physiotherapist will teach you how to use your other hand or a wall for resistance while you flex and tighten your muscles, creating an isometric contraction of the shoulder muscles. Your therapist will then progress your exercises so that you are strengthening the muscles through their available ranges of motion as you regain these motions. This may involve using light weights or Theraband to add resistance for your upper limb. Adequate strength and endurance in the rotator cuff muscles throughout a variety of ranges of motion, including over shoulder height, is needed to ensure full functioning of the shoulder.
As a result of any injury, the receptors in your joints and ligaments that assist with proprioception (joint sense of position) decline in function. A period of immobility will add to this decline. Although your arm and shoulder girdle are not traditionally thought of as weight bearing parts of the body, even an activity such as assisting yourself with your arms to get out of a chair or pulling a glass from a cupboard requires weight to be put through or lifted by your shoulder girdle and for your body to be proprioceptively aware of your limb.
The proprioceptive control of the scapula on the rib cage (scapulothoracic motion) is especially important in being able to use your shoulder girdle and upper limb effectively without causing further injury. Normal scapulothoracic motion is particularly essential once you are able to use your limb near or above shoulder height. For this reason, your Physiotherapist will teach you how to properly control your scapula during everyday activities as well as during your rehabilitation exercises. Your Physiotherapist will also remind you about maintaining good shoulder posture even when sitting or using your upper limb in activities below shoulder height, such as working on the computer.
Rounded shoulders in this position crowds the shoulder joint and can lead to or prolong shoulder impingement and pain. Regaining proprioception of the shoulder girdle and upper limb requires concentrated work, as most people have not previously needed to focus so intently on such controlled motions. The concentrated effort, however, has a substantial reward, as good scapulothoracic control is the key to avoiding further shoulder problems once your adhesive capsulitis has been rehabilitated.
Proprioceptive exercises might include activities such as rolling a ball on a surface with your hand, holding a weight up overhead in lying while you move your shoulder, or pushups on an unstable surface. Advanced exercises may include activities such as ball throwing or catching overhead once you gain that range of motion.
As mentioned above, adhesive capsulitis can unfortunately be a slow problem to resolve. You may need therapy treatments for three to four months or longer before you get full shoulder motion and function back, and you will need to also continue your home exercise programme for at least as long.
If conservative treatment at Physio Med is not progressing as quickly as your Physiotherapist would expect, then further intervention may be required.
Non-conservative treatments
Manipulation Under Anesthesia
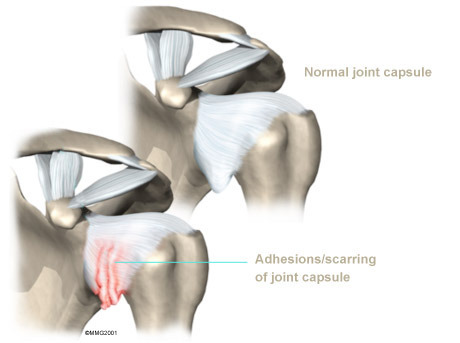
If progress in rehabilitation is slow, your doctor may recommend manipulation under anesthesia (MUA.) This means that you are put to sleep with general anesthesia. Once under the anesthesia the surgeon then aggressively stretches your shoulder joint into the ranges of motion that you were unable to achieve on your own. The heavy action of the manipulation stretches the shoulder joint capsule and breaks up the scar tissue. In most cases, the manipulation improves motion in the joint faster than allowing nature to take its course on its own. You may need this procedure done more than once.
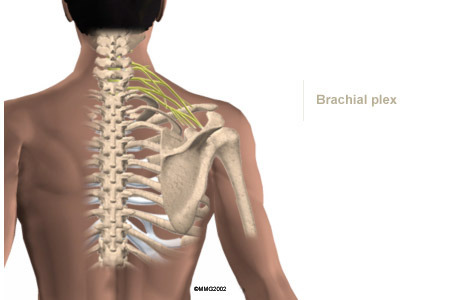
As with any procedure, MUA has risks. There is a very slight chance that the aggressive stretching can injure the nerves of the brachial plexus, which is the network of nerves running to your arm. There is also a risk of fracturing the humerus (the bone of the upper arm), especially in people who have osteopenia or osteoporosis (fragile bones).
Arthroscopic Release
When it becomes clear that Physiotherapy and MUA have not improved shoulder motion, an arthroscopic release may be needed. This procedure is usually done using an anesthesia block to deaden the arm. The surgeon then uses an arthroscope, which is a slender tube with a camera attached, to see inside the joint.
During the arthroscopic procedure, the surgeon cuts (releases) any restricting scar tissue, the ligament on top of the shoulder (coracohumeral ligament), and a small portion of the joint capsule. A biopsy of the scar tissue is also sent to the lab for evaluation to determine the stage of adhesive capsulitis. If shoulder movement is not regained or if the surgeon is unable to complete the surgery using the arthroscope, an open procedure may be needed. An open procedure requires a larger incision so the surgeon can work inside the joint more easily.
At the end of the release procedure, the surgeon gently manipulates the shoulder to gain additional motion. A steroid may also be injected into the shoulder joint at the completion of the procedure.
Nerve Block
Numbing the suprascapular nerve to the shoulder is a newer technique used in some pain clinics. This procedure can be done on an outpatient basis, which means you'll be in and out the same day. A single injection of a numbing agent combined with a steroid medication temporarily eliminates the pain signals, similar to hitting a "reset" button inside the shoulder. The nerve pathway sending continuous pain signals from the shoulder to the spinal cord and up to the brain is turned off. For a short time, the patient can move the arm without pain, and often that is enough to get the shoulder back on track for improved movement and function.
Hydrodilation
Another new technique called hyrdodilation or brisement is being used as an alternative to surgery. A fluid is injected into the joint causing the capsule to expand until the adhesions and scar tissue burst. The result can be relief of pain and improved function. Unfortunately there have not been enough studies done yet to see how well this approach really works or to determine any long-term effects of this technique. In addition, there have not been any studies comparing this technique to other more traditional techniques, such as manipulation or nerve block, to determine if it is really any more effective.
Rehabilitation after Non-conservative Treatment
What can I expect during rehabilitation after one of the above treatments?
Immediately after one of the above procedures, your surgeon may place your shoulder in a continuous passive motion (CPM) machine. CPM machines are used immediately after many different types of joint surgeries. This machine keeps the shoulder moving and alleviates joint stiffness. The machine simply straps to the arm and, as the name suggests, continuously moves the joint. This continuous motion is thought to reduce stiffness, ease pain, and keep extra scar tissue from forming inside the joint.
Some surgeons apply a dynamic splint to the shoulder after manipulation or arthroscopic surgery. A dynamic splint puts the shoulder into a full stretch and holds it in that position. Keeping the shoulder stretched gradually loosens up the joint capsule.
You'll resume Physiotherapy at Physio Med after undergoing any of the non-conservative treatment approaches. Some surgeons have their patients in therapy every day for one to two weeks. The idea of Physiotherapy so soon after the treatment is to maintain the range of motion that was gained during the procedure. The stretching also keeps new scar tissue from forming and binding the capsule again. Your Physiotherapist will also encourage you to frequently do your home exercise programme, which at this stage will mainly consist of range of motion and some proprioception exercises. A pulley will be very useful at this time to repetitively move your shoulder passively into its new range of motion. Your Physiotherapist will also encourage you to use your shoulder and arm as frequently as possible in everyday activities to also encourage range of motion. Modalities such as heat, ice, ultrasound, or electrical current may be used after the stretching to aid in pain relief.
Your shoulder movement should improve continually after the procedure and therapy. If it does not, you may unfortunately require another procedure.
The main focus of our Physiotherapy at Physio Med after having a non-conservative procedure is to maintain the range of motion gained during the procedure. Gaining full range of motion is the ultimate goal. Strength in the early stages is not as important so, typical strengthening exercises will not begin for four to six weeks after the procedure. Simple isometric exercises may be used in the early stages to maintain muscle tone, but advanced exercises with weights or Theraband will not be focused on in the early stage of rehabilitation. Advanced proprioception exercises however, as described under conservative treatment, are important very early on in your rehabilitation so will begin immediately, and will continually be focused on as the shoulder improves.
Overall you may require Physiotherapy for up to two to three months after undergoing one of the above procedures.
Our overall goal at Physio Med is to help you regain full shoulder motion, strength, and function. If you are not improving as we would expect, or your pain is not well controlled during your rehabilitation, we will ask you to return to your surgeon for follow-up to ensure there are no complicating factors impeding your recovery.
When you are well under way, regular visits to our clinic will end. Your therapist will continue to be a resource, but you will be in charge of doing your exercises as part of an ongoing home programme.
Portions of this document copyright MMG, LLC.












 Bongcawel")





















